Game five - in which I get to do some research and reminisce
But what to do. There are a number of options:
- Do nothing yet - but apply active surveillance. But I don't like the thought of spending my life worrying and I didn't enjoy one biopsy let alone one or two a year.
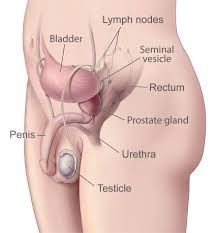
- Surgery. This is the traditional solution. In the bad old days a surgeon would make a hole big enough to see what he or she is doing then carefully remove the gland trying not to damage the urethra or the nerves to the penis - not always successfully. These days it can be more reliably done by robot, that provides much finer movements and keyhole surgery with six, relatively small, holes for the manipulators and vision devices. But in men over 70 with enlarged prostates the prognosis is not good if one wants to preserve one's remaining sexual function and avoid a bag permanently strapped to the leg to receive urine.
- Destruction of the gland by other means. These include high intensity ultrasound focussed on the target areas and a method called 'Nanoknife Focal Ablation' in which a number of electrodes are inserted around the tumour and electrical pulses passed in such a way that the abnormal tissue is destroyed but there is not excessive heating that could damage healthy surrounding tissue. Thus preserving the urethra and associated nerves. In younger men full sexual function can often be preserved. This can be done as day surgery, with little ongoing trauma, and it seemed the best of the surgical options. The only downside for me was ongoing monitoring, that includes more biopsies, to ensure that all the cancer has been removed.
- Radiation. In advanced cases this is often the only option. Traditionally, a gamma-ray source (typically the radioisotope cobalt-60) was or is rotated around the body, focussed on the tumour but also irradiating surrounding tissue, so that a large number of sessions were/are required to allow healthy tissue time to recover. The symptoms of radiation sickness may be experienced. Cobalt technology has largely been replaced by the linear-accelerator (Linac), which can generate higher-energy radiation. Cobalt treatment still has a useful role to play in certain applications and is still in widespread use worldwide, since the machinery is relatively reliable and simple to maintain compared to the modern linear-accelerator.
- A related surgical procedure is seed technology (brachytherapy) - in which a radioactive isotope, typically iodine 125 with a half life of 60 days, is inserted into the tumour in small lines like an artist's hatching. This has the benefit that the radiation is from the inside out. But it seems that my prostate is now too large for this to be done without risk (62 cm3) and it would require a course of hormone injections to reduce testosterone and shrink it. The side effects of which are unappealing.
But just as I was steeling myself to the prospect of the Nanoknife I learned that there is a brand-new machine in Sydney that seems to be the best solution of all.
It's radiation therapy: a version that incorporates the relatively new linear-accelerator technology. But what makes this machine special and ground-breaking is that the linear-accelerator is combined with a, now familiar, MRI (see above).
More physics fun:
How does radiation therapy work?
Most of us are familiar with rainbows created when water droplets refract sunlight to split it into its various wavelengths. The refraction of different wavelengths (colours) has fruitfully occupied physicists since Newton (and fascinated inquisitive humans - genus homo - for millions of years).
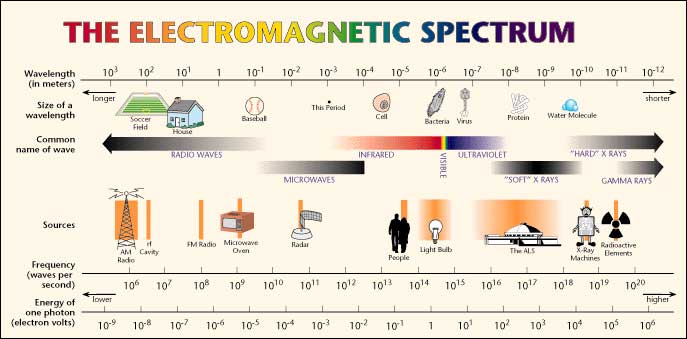
Yet it was not until 1865 that the great Scottish physicist James Clerk Maxwell in his paper 'A Dynamical Theory of the Electromagnetic Field', proposed that that light is an undulation in the same medium that is the cause of electric and magnetic phenomena and linked these in his ground breaking 'equations'. These demonstrate that there is an electromagnetic spectrum and predicted the existence of radio waves before they were discovered; as well as describing Roentgen's x-rays and Marie and Pierre Curie's 'radioactivity'.
Later experiments confirmed Maxwell's electromagnetic hypothesis but failed to find a medium (such as a luminiferous ether) in which the waves are propagated. This led Einstein to his Theory of Special Relativity and then to the realisation that matter and energy are equivalent - and thus to the atom bomb and nuclear power. Today we know radio waves; radiant heat; light; and gamma rays to all consist of photons, of increasing frequency and energy.
If we were seriously wrong about any of this then a lot of modern technology would not work so 'the proof is in the pudding'.
 Unknown author, Public domain, via Wikimedia Commons
Unknown author, Public domain, via Wikimedia Commons
Those of you familiar with Roentgens' invention (Wilhelm Roentgen, Professor of Physics in Wurzburg, Bavaria, discovered mysterious 'X'-rays in 1895), will quickly understand how to generate high frequency photons. Every museum of technology in the world has a Roentgen Tube on display somewhere. It's one of the most important inventions of all time. And it's simple.
In an evacuated glass envelope an electron beam is fired at a heavy metal (tungsten) target at 45 degrees, causing the outer electron shells of the tungsten metal atoms to change energy states and emit photons (x-rays - electromagnetic radiation) at roughly 90 degrees to the electron beam (it's all about Fermions (electrons) and Bosons (photons)). Or just think of a splash formed by throwing a stone into a pond.
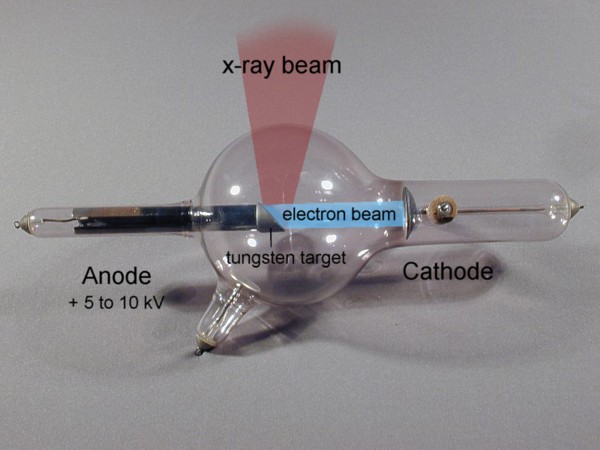 X-ray tube, type 'Gundelach' 1896 - from http://physik.uibk.ac.at/museum - with my labels and graphic additions
X-ray tube, type 'Gundelach' 1896 - from http://physik.uibk.ac.at/museum - with my labels and graphic additions
If you have ever had an x-ray of your chest a broken bone or your mouth x-rayed at the dentist, this simple device, or a modern variation, was the source of the radiation. Someone skilled in glasswork and having a good vacuum pump and a high voltage power supply could knock one up in their back shed.
X-rays (and higher energy photons) are what is known as 'ionising radiation' that is they are sufficiently powerful to knock an electron out of an atom causing a short lived chain reaction (Compton radiation). If that atom happens to be in one of your cells and other atoms are impacted too, this has the potential to kill that cell or alter its DNA. Of course you have plenty of cells - around thirty seven thousand billion in an adult human of which around around three quarters of a million die and are replaced every second as a result of natural processes. See The Chemistry of Life on this website)
So statistically the odds are quite good that nothing nasty will happen; but not so good that one should go about having unnecessary x-rays and bumping off or altering cells willy-nilly.
Yet for a period x-ray machines became ubiquitous. When I was a child we even had them in shoe shops to see if your new shoes fitted correctly. We also had houses built of asbestos sheeting and used DDT to kill flies in our homes. Lots of dangerous fun and games. Yet we now live longer - who knew?
But ordinary 'soft' x-rays aren't much good at deliberately killing lots of cells. For that you need much more energetic photons like those emitted by radioactive cobalt-60, manufactured in a nuclear reactor.
This can also be achieved by striking the heavy metal (usually tungsten alloy) target with much more energetic electrons.
Those of you who knew how your old your cathode-ray tube TV or computer monitor worked will be familiar with the electron guns at the rear. If, instead of painting a picture on phosphor, a similar electron beam is repeatedly boosted in energy, the final electron beam can be used to generate ever more energetic photons - gamma-rays.
In a linear accelerator adding energy (velocity - you know E=MV2) to electrons is achieved by a sequence of ever lengthening tubular electrodes, excited to alternate in polarity, pulling then pushing (opposite polarities attract equivalents repel), at microwave frequency derived from a magnetron and an associated wave guide (like the active device in a microwave oven).
 Chetvorno, CC0, via Wikimedia Commons - in this case single positive particles are depicted
Chetvorno, CC0, via Wikimedia Commons - in this case single positive particles are depicted
In our case large bundles of electrons are accelerated by similar means
At each electrode the electron beam absorbs more energy from the magnetron. When the beam is sufficiently energetic (typically from 4 to 25 MeV) it's turned and aimed at the tungsten target to produce photons. The resulting photon beam has similar energy to the electron beam (less some heat), well above x-ray, to gamma-ray frequency. At each increase in electron energy the ionising potential of the resulting photons increases. The resulting gamma radiation has the ability to excite the electrons of hydrogen atoms, breaking the bonds that bind proteins, and thus to destroy the cells that form living tissue.
The energy of the gamma radiation produced by a Linac substantially exceeds that emitted by radioactive isotopes like cobalt-60 (around 1.25 MeV), yet can be turned on and off just as quickly as any x-ray machine and is tuneable in terms of energy and thus frequency.
This is a really good game. Lot's of fun for physicists and engineers.
Now that we have a beam how do we use it? It's a blunt instrument until its shaped and focussed onto the target cells. We could just point it at a tumour and stay on it until the tumour was dead but then we would have a tunnel of dead tissue in my case in through the front and out my back as if I'd been shot. I would not be at all well. So the trick is to shoot less harmful bursts of photons from lots of different angles all passing through a common point, where the tumour exists so that the cumulative impact at that point is most deadly; while collateral damage is reduced.
Originally the beam produced by these machines was like that produced by a flashlight, perhaps shaded to one side, but tumours are not always regular and from some angles important organs could be collateral damage.
So it was soon realised that changing the shape of the beam for example to go between important organs would be advantageous. This is the role of the multi-leaf collimator. These consist of around sixty pairs of opposed metal plates or leaves; arranged face to face, with their narrow side towards the beam. Each is wide enough to block a gamma ray photon (around 7cm of tungsten alloy). By sliding the leaves into the beam they shape the aperture to any required. Thus by programming a computer, that controls the leaf activating motors, the beam can be shaped to conform to the shape of the tumour, as seen from each individual angle of attack. This is called planning.
But it's tricky, unless the planning computer has an accurate MRI scan in full three dimensions so that it can work out which shape to make the beam at any angle of attack and what angles to avoid, as they could damage sensitive surrounding organs. Further, patients have to be in exactly same position as they were in the MRI scanner or the plan will be problematic.
Why not combine the two? Here the engineers came to the rescue.
Thus when a high powered linear-accelerator is combined in a suitable MRI scanner a tumour can now be targeted with millimetre accuracy, in real-time, in the same machine. The risk to surrounding tissue is very much reduced and just five sessions are typically sufficient to destroy a tumour, with considerable confidence, so that, in the case of a prostate tumour, on-going monitoring is limited to regular PSA checks.