We all die of something.
After 70 it's less likely to be as a result of risky behaviour or suicide and more likely to be heart disease followed by a stroke or cancer. Unfortunately as we age, like a horse in a race coming up from behind, dementia begins to take a larger toll and pulmonary disease sees off many of the remainder. Heart failure is probably the least troublesome choice, if you had one, or suicide.
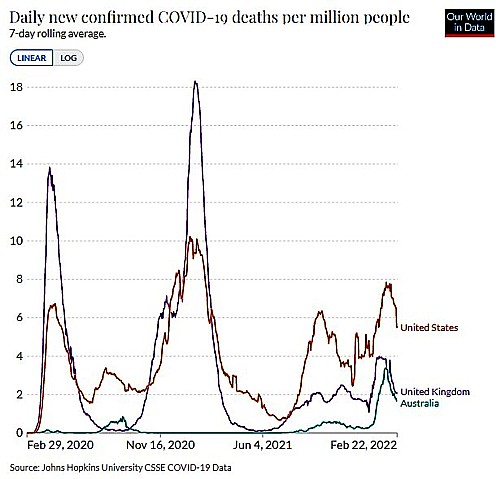
In 2020 COVID-19 has become a significant killer overseas but in Australia less than a thousand died and the risk from influenza, pneumonia and lower respiratory conditions had also fallen as there was less respiratory infection due to pandemic precautions and increased influenza immunisation. So overall, in Australia in 2020, deaths were below the annual norm. Yet 2021 will bring a new story and we've already had a new COVID-19 hotspot closing borders again right before Christmas*.
So what will kill me?
Some years back, in October 2016, at the age of 71, my aorta began to show it's age and I dropped into the repair shop where a new heart valve - a pericardial bio-prosthesis - was fitted. See The Meaning of Death elsewhere on this website. This has reduced my chances of heart failure so now I need to fear cancer; and later, dementia.
More fun and games.
Game one - in which my PSA has suddenly risen
One of the main killers of men is prostate cancer. When men of 'a certain age' get an annual blood test one indicator typically checked, along with cholesterol and so on, is our PSA (prostate specific antigen) value.
Many men have their prostate removed, so clearly one can do without it.
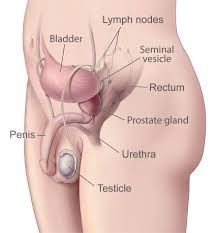
"Hey Google," I asked: "What's this prostate for anyway?"
Her dulcet voice told me: "The prostate gland (the prostate) is an organ of the male reproductive system. It is about the size of a walnut and is found at the base of the bladder. The thin tube that allows urine and semen to pass out of the penis (the urethra) runs through the prostate gland. Alkaline fluid produced by the prostate gland helps to nourish sperm and leaves the urethra as ejaculate (semen)..."
Prostate cancer is the most common of these but can be slow in advancing so it is famously the one 'that most men die with, rather than die of'. A PSA test provides a clue but can be unreliable. Nevertheless, when it suddenly starts rising it may indicate that a further check would be prudent.
Game two - in which I lie down in a tunnel
Fortunately these days magnetic resonance imaging (MRI) scanners, once leading edge technology, are relatively ubiquitous and are quite good at identifying clusters of abnormal cells - tumours.
These machines subject one to a succession of very high magnetic pulses (typically 1.5 or 3 teslas (T)).
High magnetic fields are relatively harmless to humans - unlike x-rays.
As it is relatively harmless, the process can take a lot longer than a computed axial tomography (CAT) scan, that employs x-rays (in a similar looking machine) and thus MRI generates superior images for organ differentiation and tumour identification - tumours that a CAT scan may not see.
In order to achieve the very high magnetic flux required, coils of superconducting wire (niobium-titanium or niobium-tin) are used and these must be cooled using liquid helium (4.2 degrees above absolute zero).
As long as one is not claustrophobic there is no sensation except for the loud noise generated by the pulsing of superconducting coils and in some machines the helium pump that delivers liquid helium to cool the coils. Ear protection and music is provided so that it can be pleasantly relaxing. Perhaps like one of those immersion tanks provided by spas?
An MRI scan turns out to be very interesting physics and quite good fun.
How does it work?
I suppose everyone with a basic education knows that the nucleus of an atom consists of protons (positively charged particles) and neutrons (having mass but no charge). Thus the charge carried by a nucleus may be more to one side than the other. Under a strong magnetic field these nuclei and therefore their atoms and molecules will try to line up, like iron filings with a magnet. Atoms and molecules that are magnetically polar, as a result of the arrangement of protons in their nucleus (like hydrogen and therefore water), are momentarily rotated by the magnetic flux, then spring back. The effect varies according to the arrangement of molecules and therefore the type of body cell
These events can be observed using radio waves, as in radar. To do this harmless microwave frequency radio waves, think of Bluetooth on your phone, bathe the patient and interact with the aforesaid atoms, molecules and cells. Externally placed antennas receive returned radio waves to build a map of a cross sections of the patient's body, as if sliced, to reveal one's vitals, in a similar way to those produced by the familiar radar scanners used in boats and aircraft.
The main limitation on an MRI scan is the need to exclude any ferromagnetic metals or metallic loops in which high currents could be induced. Things like watches jewellery and heart pacemakers can be destroyed. Those with such devices must not approach the machine. Warnings of imminent death for pacemaker wearers abound.
Game three - in which a possible tumour is identified
Despite my initial scepticism and inclination to disregard the PSA result the MRI found a suspicious area in my prostate, at this stage still localised.
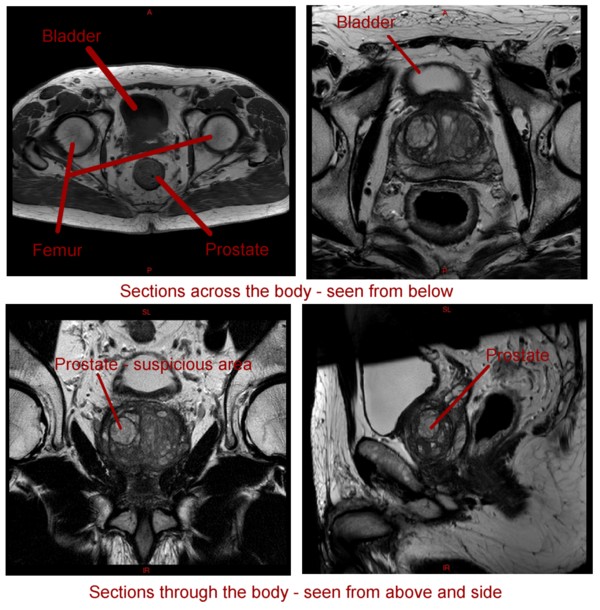 My own images and notation from I-Med Radiology MRI scans
My own images and notation from I-Med Radiology MRI scans
So what should I do? My first reaction was to wait and then get another MRI scan, in say a year to see if it has grown. But if I did would I spend a year worrying. And what if the tumour is aggressive and doubles or worse metastasises and spreads to other organs?
Game four - in which I get a needle inserted through my perineum and I die (again)
The perineum is the area between the penis and the anus and it's adjacent to the prostate. Once through the perineum the sampling needle is repeatedly stabbed into the prostate, as if it were a pin cushion, to extract cells from its different regions. This is done using an ultrasound probe in the anus, to image the process, and with the patient under a total anaesthetic - unaware.
So I lay on a hospital trolley, a cannula was inserted by a pleasant woman and everything went black - dead again - until I heard an angelic voice: "Richard! wake up."
So I had to rely on Wikipedia to find out what happened:
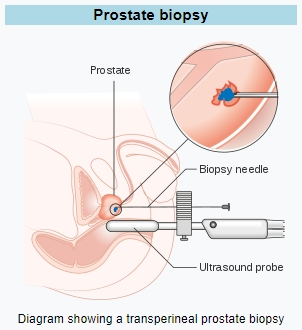 Cancer Research UK <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
Cancer Research UK <https://creativecommons.org/licenses/by-sa/4.0>, via Wikimedia Commons
There was no pain - analgesics not required - but it was uncomfortable - and no where near as much fun as the scanner. And I was passing blood in my urine for around two weeks. Julia was unsympathetic: "young women suffer that every month," she told me.
I was still confident it would all be a wild goose chase. But then the surgeon called me: "You have a left mid-post-lateral tumour (Gleeson 4+3) and while it is not critically urgent you need to do something about it soon. Sometime within the next three months would be a good idea."
Game five - in which I get to do some research and reminisce
But what to do. There are a number of options:
- Do nothing yet - but apply active surveillance. But I don't like the thought of spending my life worrying and I didn't enjoy one biopsy let alone one or two a year.
- Surgery. This is the traditional solution. In the bad old days a surgeon would make a hole big enough to see what he or she is doing then carefully remove the gland trying not to damage the urethra or the nerves to the penis - not always successfully. These days it can be more reliably done by robot, that provides much finer movements and keyhole surgery with six, relatively small, holes for the manipulators and vision devices. But in men over 70 with enlarged prostates the prognosis is not good if one wants to preserve one's remaining sexual function and avoid a bag permanently strapped to the leg to receive urine.
- Destruction of the gland by other means. These include high intensity ultrasound focussed on the target areas and a method called 'Nanoknife Focal Ablation' in which a number of electrodes are inserted around the tumour and electrical pulses passed in such a way that the abnormal tissue is destroyed but there is not excessive heating that could damage healthy surrounding tissue. Thus preserving the urethra and associated nerves. In younger men full sexual function can often be preserved. This can be done as day surgery, with little ongoing trauma, and it seemed the best of the surgical options. The only downside for me was ongoing monitoring, that includes more biopsies, to ensure that all the cancer has been removed.
- Radiation. In advanced cases this is often the only option. Traditionally, a gamma-ray source (typically the radioisotope cobalt-60) was or is rotated around the body, focussed on the tumour but also irradiating surrounding tissue, so that a large number of sessions were/are required to allow healthy tissue time to recover. The symptoms of radiation sickness may be experienced. Cobalt technology has largely been replaced by the linear-accelerator (Linac), which can generate higher-energy radiation. Cobalt treatment still has a useful role to play in certain applications and is still in widespread use worldwide, since the machinery is relatively reliable and simple to maintain compared to the modern linear-accelerator.
- A related surgical procedure is seed technology (brachytherapy) - in which a radioactive isotope, typically iodine 125 with a half life of 60 days, is inserted into the tumour in small lines like an artist's hatching. This has the benefit that the radiation is from the inside out. But it seems that my prostate is now too large for this to be done without risk (62 cm3) and it would require a course of hormone injections to reduce testosterone and shrink it. The side effects of which are unappealing.
But just as I was steeling myself to the prospect of the Nanoknife I learned that there is a brand-new machine in Sydney that seems to be the best solution of all.
It's radiation therapy: a version that incorporates the relatively new linear-accelerator technology. But what makes this machine special and ground-breaking is that the linear-accelerator is combined with a, now familiar, MRI (see above).
More physics fun:
How does radiation therapy work?
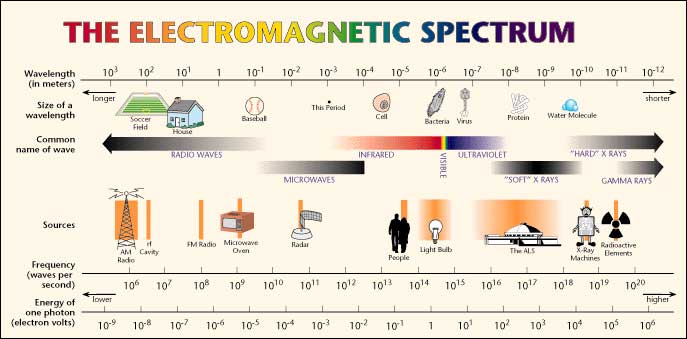
Most of us are familiar with rainbows created when water droplets refract sunlight to split it into its various wavelengths. The refraction of different wavelengths (colours) has fruitfully occupied physicists since Newton (and fascinated inquisitive humans - genus homo - for millions of years).
Yet it was not until 1865 that the great Scottish physicist James Clerk Maxwell in his paper 'A Dynamical Theory of the Electromagnetic Field', proposed that that light is an undulation in the same medium that is the cause of electric and magnetic phenomena and linked these in his ground breaking 'equations'. These demonstrate that there is an electromagnetic spectrum and predicted the existence of radio waves before they were discovered; as well as describing Roentgen's x-rays and Marie and Pierre Curie's 'radioactivity'.
Later experiments confirmed Maxwell's electromagnetic hypothesis but failed to find a medium (such as a luminiferous ether) in which the waves are propagated. This led Einstein to his Theory of Special Relativity and then to the realisation that matter and energy are equivalent - and thus to the atom bomb and nuclear power. Today we know radio waves; radiant heat; light; and gamma rays to all consist of photons, of increasing frequency and energy.
If we were seriously wrong about any of this then a lot of modern technology would not work so 'the proof is in the pudding'.
 Unknown author, Public domain, via Wikimedia Commons
Unknown author, Public domain, via Wikimedia Commons
Those of you familiar with Roentgens' invention (Wilhelm Roentgen, Professor of Physics in Wurzburg, Bavaria, discovered mysterious 'X'-rays in 1895), will quickly understand how to generate high frequency photons. Every museum of technology in the world has a Roentgen Tube on display somewhere. It's one of the most important inventions of all time. And it's simple.
In an evacuated glass envelope an electron beam is fired at a heavy metal (tungsten) target at 45 degrees, causing the outer electron shells of the tungsten metal atoms to change energy states and emit photons (x-rays - electromagnetic radiation) at roughly 90 degrees to the electron beam (it's all about Fermions (electrons) and Bosons (photons)). Or just think of a splash formed by throwing a stone into a pond.
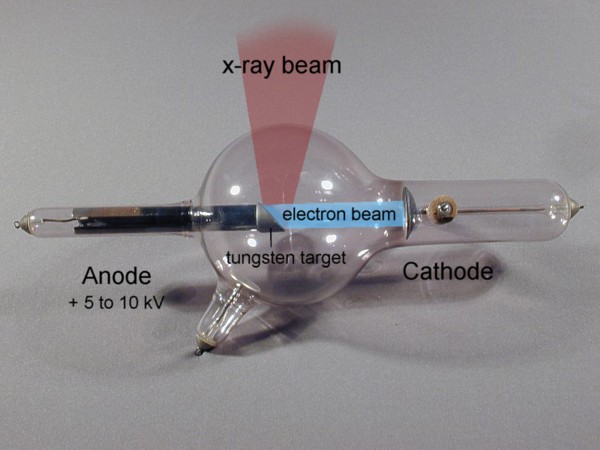 X-ray tube, type 'Gundelach' 1896 - from http://physik.uibk.ac.at/museum - with my labels and graphic additions
X-ray tube, type 'Gundelach' 1896 - from http://physik.uibk.ac.at/museum - with my labels and graphic additions
If you have ever had an x-ray of your chest a broken bone or your mouth x-rayed at the dentist, this simple device, or a modern variation, was the source of the radiation. Someone skilled in glasswork and having a good vacuum pump and a high voltage power supply could knock one up in their back shed.
X-rays (and higher energy photons) are what is known as 'ionising radiation' that is they are sufficiently powerful to knock an electron out of an atom causing a short lived chain reaction (Compton radiation). If that atom happens to be in one of your cells and other atoms are impacted too, this has the potential to kill that cell or alter its DNA. Of course you have plenty of cells - around thirty seven thousand billion in an adult human of which around around three quarters of a million die and are replaced every second as a result of natural processes. See The Chemistry of Life on this website)
So statistically the odds are quite good that nothing nasty will happen; but not so good that one should go about having unnecessary x-rays and bumping off or altering cells willy-nilly.
Yet for a period x-ray machines became ubiquitous. When I was a child we even had them in shoe shops to see if your new shoes fitted correctly. We also had houses built of asbestos sheeting and used DDT to kill flies in our homes. Lots of dangerous fun and games. Yet we now live longer - who knew?
But ordinary 'soft' x-rays aren't much good at deliberately killing lots of cells. For that you need much more energetic photons like those emitted by radioactive cobalt-60, manufactured in a nuclear reactor.
This can also be achieved by striking the heavy metal (usually tungsten alloy) target with much more energetic electrons.
Those of you who knew how your old your cathode-ray tube TV or computer monitor worked will be familiar with the electron guns at the rear. If, instead of painting a picture on phosphor, a similar electron beam is repeatedly boosted in energy, the final electron beam can be used to generate ever more energetic photons - gamma-rays.
In a linear accelerator adding energy (velocity - you know E=MV2) to electrons is achieved by a sequence of ever lengthening tubular electrodes, excited to alternate in polarity, pulling then pushing (opposite polarities attract equivalents repel), at microwave frequency derived from a magnetron and an associated wave guide (like the active device in a microwave oven).
 Chetvorno, CC0, via Wikimedia Commons - in this case single positive particles are depicted
Chetvorno, CC0, via Wikimedia Commons - in this case single positive particles are depicted
In our case large bundles of electrons are accelerated by similar means
At each electrode the electron beam absorbs more energy from the magnetron. When the beam is sufficiently energetic (typically from 4 to 25 MeV) it's turned and aimed at the tungsten target to produce photons. The resulting photon beam has similar energy to the electron beam (less some heat), well above x-ray, to gamma-ray frequency. At each increase in electron energy the ionising potential of the resulting photons increases. The resulting gamma radiation has the ability to excite the electrons of hydrogen atoms, breaking the bonds that bind proteins, and thus to destroy the cells that form living tissue.
The energy of the gamma radiation produced by a Linac substantially exceeds that emitted by radioactive isotopes like cobalt-60 (around 1.25 MeV), yet can be turned on and off just as quickly as any x-ray machine and is tuneable in terms of energy and thus frequency.
This is a really good game. Lot's of fun for physicists and engineers.
Now that we have a beam how do we use it? It's a blunt instrument until its shaped and focussed onto the target cells. We could just point it at a tumour and stay on it until the tumour was dead but then we would have a tunnel of dead tissue in my case in through the front and out my back as if I'd been shot. I would not be at all well. So the trick is to shoot less harmful bursts of photons from lots of different angles all passing through a common point, where the tumour exists so that the cumulative impact at that point is most deadly; while collateral damage is reduced.
Originally the beam produced by these machines was like that produced by a flashlight, perhaps shaded to one side, but tumours are not always regular and from some angles important organs could be collateral damage.
So it was soon realised that changing the shape of the beam for example to go between important organs would be advantageous. This is the role of the multi-leaf collimator. These consist of around sixty pairs of opposed metal plates or leaves; arranged face to face, with their narrow side towards the beam. Each is wide enough to block a gamma ray photon (around 7cm of tungsten alloy). By sliding the leaves into the beam they shape the aperture to any required. Thus by programming a computer, that controls the leaf activating motors, the beam can be shaped to conform to the shape of the tumour, as seen from each individual angle of attack. This is called planning.
But it's tricky, unless the planning computer has an accurate MRI scan in full three dimensions so that it can work out which shape to make the beam at any angle of attack and what angles to avoid, as they could damage sensitive surrounding organs. Further, patients have to be in exactly same position as they were in the MRI scanner or the plan will be problematic.
Why not combine the two? Here the engineers came to the rescue.
Thus when a high powered linear-accelerator is combined in a suitable MRI scanner a tumour can now be targeted with millimetre accuracy, in real-time, in the same machine. The risk to surrounding tissue is very much reduced and just five sessions are typically sufficient to destroy a tumour, with considerable confidence, so that, in the case of a prostate tumour, on-going monitoring is limited to regular PSA checks.
Game six - in which I'm on my back in a tunnel again
So now I'm getting ready for the beam to be turned on. Before each session I have to fast for several hours and drink lot's of water. I've had my initial introduction to the MR-Linac.
 Image from: https://www.genesiscare.com/au/mrl-hcp/
Image from: https://www.genesiscare.com/au/mrl-hcp/
|
The picture shows the: 1.5 T MRI scanner (yellow); the magnetron and associated linear accelerator (black); joined by the white tube where the electrons are magnetically turned into the target apparatus, (black); where the gamma-ray photons are produced; and, near the MRI, the 'multileaf collimator'; where the photon beam is shaped before entering the patient. From the News Release: July 22, 2020 – Elekta (EKTA-B.ST) announced today that the GenesisCare oncology centre at St. Vincent’s Hospital (Sydney, New South Wales) has started treating patients with Elekta Unity, a radiation therapy system that allows doctors to see a tumour's movements and its exact position during the delivery of therapeutic radiation. St. Vincent’s is the first site of 21 eventual Elekta Unity installations in GenesisCare’s global network to initiate clinical use of the system... |
I get the feeling that it's still a new toy. Everyone is committed; professional; and very careful. But then, that's been my experience on every hospital visit to date. "We have a very good healthcare system," I think to myself.
The first day I spent about an hour in the tunnel (or so it seemed) and was scanned a couple of times to get used to it then I went across to the CAT scanner where three tiny markers were tattooed above my prostate (in my pubic area) and on my hips (at the side) so that I can be repeatedly put in exactly the same position.
More fun - I don't mind a CAT scan - just another x-ray - child's play compared to a gamma beam.
The next session was a dry planning run of an actual treatment session with just the MRI. As it turned out, not so dry, thanks to all that water.
On my third day in the machine, after well over an hour of setup and planning, the 7 MeV gamma beam became active and cells began to die. Did I imagine a slight tingling or a twinge or two? Possibly. But it's quite loud with the simultaneous MRI so I can't be sure. It was certainly not painful.
The following day I was feeling slightly down emotionally and a little nauseous. Was it as a result of the radiation; or was it because it was raining and miserable, curtailing my usual morning walk? After my third treatment I was in no doubt. The radiation was certainly doing something! My bladder and bowels were a mess.
That's when this game suddenly became real.
My final treatment was on the last day of that 'annus horribilis' 2020. Although I wasn't feeling chipper I was able to drive to our friends' house and enjoy a fine meal and watch the fireworks on TV, to bring in the New Year, while hearing them boom outside. The next day wasn't so good. I didn't get out but on the 2nd January got up and walked to the shops (putting on my mask as is now required*).
| *COVID-19 hotspot
The latest COVID-19 outbreak originated around Newport on the northern beaches, thanks to someone recently arrived from the US (it's a US strain) successfully dodging quarantine. Aircrew who have less supervision, and have been trusted to isolate, are suspected. There are now reports of past aircrew breaches, occasioning several, thousand dollar, fines. Yet the cost of this breach will be in the tens of millions as clubs, pubs and cafés are closed and the entire northern beaches area is in lock-down, right before Christmas. Many people's Christmas celebrations in Sydney; and all interstate holiday travel; and New Year's eve fireworks watching; have been ruined. Trust in aircrew has abruptly ended. From now on they will be kept in guarded hotels like everyone else in quarantine. But it's shutting the stable gate after the colt has bolted. Let's hope he hasn't hasn't joined the wild bush horses already. Thanks to Middle Harbour, Mosman has not been affected by the full lockdown - just increased caution and no travel across the Spit bridge. While this has got the northern beaches under control there are now isolated cases elsewhere, including in Victoria (the same northern beaches/US strain) Updates to follow.
|
It's 12 days since my last treatment. I walked down to the beach again and I'm almost back to normal. I suspect that I'm in better shape than I might have been under any of the other options. And its far more interesting.
So if any of my readers find that they have a prostate tumour I can recommend this treatment option if it's available to you. Remembering that every case is different.
Just over a Year later (February 2022)
As a result of this treatment I suffered very few minor side-effects my bladder and bowel were very slightly burnt (?) and soon recovered entirely. Ten months after treatment my PSA that had fallen from 8% to 0.73% rose slightly to 2.2% causing some alarm and resulting in my undergoing a PET scan (reported elsewhere on this website Read More...). This proved to be clear and my PSA soon fell back to the previous very low count.
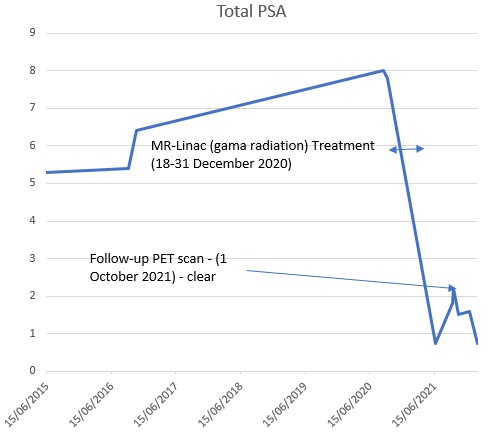
So, so far, the MR-Linac treatment has been an unequivocal success.
The Pandemic
A year ago I commented on the COVID-19 pandemic and promised an update. So, here it is.
| COVID-19 update (end February 2022)
COVID-19 restrictions are now being eased, in order to restore normal economic activity. Theatres, pubs, concerts, and schools are now free of social distancing limits and within days face-masks will also be optional. For a period, after that reported above, the virus spread to western Sydney causing extensive lock-downs. After a slow start, double vaccination rates soon exceeded 90% of the eligible population in our State and now many children are also vaccinated and about half the population has received a booster. Australia's borders have been quarantined and international travel curtailed but in June 2021 we were able to travel to Central Australia (see elsewhere on this website) and despite repeated outbreaks the principal impact at the height of the pandemic was the closure of many entertainment venues; the requirement, for many, to work-from-home and the, somewhat arduous, home-schooling of children. During 2021 I attended different hospitals on several occasions and on none of these seemed unusually overwhelmed by COVID-19 patients. Elective surgery, that was interrupted for a period, is now restored, for example: for a friend who has recently undergone a hip replacement. When the infection rate was low QR codes at all retailers and other venues enabled comprehensive contact-tracing. But a new more infectious variant (omicron) soon overwhelmed the tracing teams and has spread widely. Mainly thanks to vaccination, COVID-19 is no longer particularly deadly and Australian governments have followed the world trend towards accepting a small rise in deathrate as herd-immunity is achieved.
The continued higher daily death rates per million in the US and UK are due to wider spread of the virus, as a result of earlier mismanagement, and to lower rates of vaccination due to the activities of anti-vaxxers. Thanks to intergovernmental cooperation and coordination, total Australian COVID-19 deaths, since the start of the pandemic, have been very low by international standards (just over five thousand have died to date). Again thanks to ongoing vaccination (boosters), the daily rate is now declining, in spite of reduced restrictions (now a 7 day average of 43 per day, down from a peak of 86, Australia wide). About half these deaths are among the unvaccinated or partially vaccinated. Deaths in Australia, from all causes, prior to the pandemic, averaged about 450 a day (164,000 pa). Many of these were in the same (at risk and elderly) cohort of people who are now being killed by, or are dying with, the virus. Thus, so far, the virus has had very little impact on the overall Australian deathrate. The main impacts have been economic and social. In the absence of another more deadly variant, it appears that many countries, including Australia, are now approaching herd-immunity, enabling Australia to remove travel restrictions (quarantine) and open-up once more.
|